I have been catching up with old friends lately. Mostly through Facebook, but also through emails and other correspondence.
I am impressed with the level of success that my friends have obtained.
JB, a friend from Sunday School and Church, is now the Dean of Admissions for a large, Division 1 university.
TG, an old bicycling friend, is now a recognized figure in the "fit" movement, and a big part of Tony Horton's P90X program, and has been featured in videos and blogs and such. (His work has inspired me to become "unfat" as I like to say.)
RL is an old partner of mine from the renal roundup days. He is now a physician in the New York City area.
GK, another friend from Sunday School, now runs his own healthcare supply corporation, and travels all across the country, making money and playing golf.
HG, an old classmate, is a very successful lawyer, and political activist. He always has my support if he decides to run.
KA, my pizza-making buddy from high school, is making quite the career for himself in EMS.
Bubba, my college golf buddy, is now making a killing on the PGA Tour, and I look forward to seeing his continued success. He really does hit the ball a long way. Even if he does use pink shafts...
I'm very impressed by the success of my friends. I am glad to know them, and glad to see them mature into the leaders in their respective fields.
That's all for now.
Wednesday, September 21, 2011
Good advice
On the advice of my good friend, and trusted colleague, Flash Larry, I decided to remove the previous post.
While I stand by what was said in my post, his assertion that such comments might not be in my best interest is a good one.
Perhaps I will revisit the previous post in the future, but it will be done in a more tactful way.
I still know that I was right, and the complaint was baseless and ill conceived.
Flash Larry is a smart guy.
While I stand by what was said in my post, his assertion that such comments might not be in my best interest is a good one.
Perhaps I will revisit the previous post in the future, but it will be done in a more tactful way.
I still know that I was right, and the complaint was baseless and ill conceived.
Flash Larry is a smart guy.
Saturday, September 17, 2011
I see dead people
This post arose from a discussion I had with a colleague. I was being singled out, and essentially berated, for terminating resuscitation efforts on an 87 year old man who died while his wife was in church. His wife agreed, as did the physician on the phone. I was at the hospital after obtaining the physician's order signature to terminate resuscitation.
My colleague stated "people aren't dead until they are in a hospital, and a doctor says they are dead."
My colleague is an idiot, and thankfully, does not wear the same patch as I do, and does not serve in a primary caregiver role.
He is of the thinking that there is "something that they can do" that we can't. Like open cardiac massage on a 60-something year old patient? Hardly. This job is nothing like television makes it out to be. (Did anyone ever get pooped on during an episode of E.R.?)
Death is the most unavoidable part of life. From the moment we are born, or from the moment we are conceived, depending on your political leanings, we are destined to die.
The CDC reported 2,436,652 deaths in 2008. Only 170,314 of those were attributed to "Accidents (unintentional injuries) Intentional self-harm (suicide) and Assault (Homicide). We are ten times more likely to die from heart disease or cancer. Interestingly enough, Blacks have a much higher infant mortality rate, more than twice that of whites.
EMS responds every day to people not breathing, and without a pulse. Out-of-hospital cardiac arrest has, for lack of a better term, a terrible prognosis. On the high end of the prognosis, 8% of patients in prehospital cardiac arrest survive to discharge, while the low end cites a percentage of 2. The prognosis for in-hospital cardiac arrests are much higher, but still gravely low. One could argue for the importance of early defibrillation, and the access to healthcare providers in the hospital. (Even the janitors at my local hospital have CPR certification.)
Patients presenting in the prehospital system with either ventricular fibrillation or pulseless ventricular tachycardia have a 10-15 times greater chance of survival.
These are statistics from one source, the CDC. I doubt you would find a prehospital provider that would argue with these statistics, however. Personally, in my years of experience, I have seen a total of 2 patients who presented initially in ventricular fibrillation survive to hospital discharge, 2 patients who presented in pulseless ventricular tachycardia, and 0 who presented in a pulseless electrical activity (PEA, EMD, Ventricular escape, whatever...) survive past the emergency room. I could not tell you how many cardiac arrest calls I have run, but I would venture to say it is well over 200, which would be in line with the (admittedly doubtful) Wikipedia article.
Transporting patients without perfusing rhythms is fruitless. It does nothing but provide false hope for family members, increase the risks of accident enroute to the hospital, and increase the opportunity for injury to a provider in the back of the ambulance.
As mentioned by a person much smarter than I, "asystole is not a workable rhythm, it is a confirmation of death."
Granted, there are times to perform CPR and transport these patients to a hospital. The elderly person who collapses at the Sunday buffet is a good example. It simply wouldn't be prudent to leave a dead body covered by a sheet in front of the salad line.
There are also times in which transport is not warranted. The person in cardiac arrest, with a patent airway and intravenous access, with no signs of life, and no response to pharmacological intervention should, with family concurrence, have efforts terminated on scene.
Medical directors who insist their medics continue to transport dead people emergency to the closest hospital do nothing to advance this field. Medics who are not ready to challenge those medical directors are doing nothing for the field either.
We, as a whole, should stop transporting dead people to the hospital, only for a physician to confirm what we already know.
My colleague is still an idiot.
My colleague stated "people aren't dead until they are in a hospital, and a doctor says they are dead."
My colleague is an idiot, and thankfully, does not wear the same patch as I do, and does not serve in a primary caregiver role.
He is of the thinking that there is "something that they can do" that we can't. Like open cardiac massage on a 60-something year old patient? Hardly. This job is nothing like television makes it out to be. (Did anyone ever get pooped on during an episode of E.R.?)
Death is the most unavoidable part of life. From the moment we are born, or from the moment we are conceived, depending on your political leanings, we are destined to die.
The CDC reported 2,436,652 deaths in 2008. Only 170,314 of those were attributed to "Accidents (unintentional injuries) Intentional self-harm (suicide) and Assault (Homicide). We are ten times more likely to die from heart disease or cancer. Interestingly enough, Blacks have a much higher infant mortality rate, more than twice that of whites.
EMS responds every day to people not breathing, and without a pulse. Out-of-hospital cardiac arrest has, for lack of a better term, a terrible prognosis. On the high end of the prognosis, 8% of patients in prehospital cardiac arrest survive to discharge, while the low end cites a percentage of 2. The prognosis for in-hospital cardiac arrests are much higher, but still gravely low. One could argue for the importance of early defibrillation, and the access to healthcare providers in the hospital. (Even the janitors at my local hospital have CPR certification.)
Patients presenting in the prehospital system with either ventricular fibrillation or pulseless ventricular tachycardia have a 10-15 times greater chance of survival.
These are statistics from one source, the CDC. I doubt you would find a prehospital provider that would argue with these statistics, however. Personally, in my years of experience, I have seen a total of 2 patients who presented initially in ventricular fibrillation survive to hospital discharge, 2 patients who presented in pulseless ventricular tachycardia, and 0 who presented in a pulseless electrical activity (PEA, EMD, Ventricular escape, whatever...) survive past the emergency room. I could not tell you how many cardiac arrest calls I have run, but I would venture to say it is well over 200, which would be in line with the (admittedly doubtful) Wikipedia article.
Transporting patients without perfusing rhythms is fruitless. It does nothing but provide false hope for family members, increase the risks of accident enroute to the hospital, and increase the opportunity for injury to a provider in the back of the ambulance.
As mentioned by a person much smarter than I, "asystole is not a workable rhythm, it is a confirmation of death."
Granted, there are times to perform CPR and transport these patients to a hospital. The elderly person who collapses at the Sunday buffet is a good example. It simply wouldn't be prudent to leave a dead body covered by a sheet in front of the salad line.
There are also times in which transport is not warranted. The person in cardiac arrest, with a patent airway and intravenous access, with no signs of life, and no response to pharmacological intervention should, with family concurrence, have efforts terminated on scene.
Medical directors who insist their medics continue to transport dead people emergency to the closest hospital do nothing to advance this field. Medics who are not ready to challenge those medical directors are doing nothing for the field either.
We, as a whole, should stop transporting dead people to the hospital, only for a physician to confirm what we already know.
My colleague is still an idiot.
Friday, September 16, 2011
A what plan?
20 something female, pregnant, having contractions. These are usually lame calls.
I mean, you've known for how many weeks you would need a ride to the hospital? One would think you could save enough money for cab fare in 40 weeks. But ambulances are free.
This is a nice neighborhood, where kids go to private schools. This call is getting lamer.
Met by a nice, well dressed gentleman who directs us upstairs, to his wife, who is allegedly having contractions. I say allegedly, because I'm not sure if she is having contractions, or simply auditioning for a dying walrus.
She hands my partner a 2 inch, pink binder.
"This is my birthing plan. I want to make sure it gets to the hospital with me."
"Excuse me, what? A what plan?"
"My birthing plan. I want to make sure everything goes the way I want it."
"Was going to the hospital by ambulance part of your birthing plan?" (Hey, I'm just curious.)
"Well, no. That part wasn't in the plan."
The binder doesn't make it with us. We forgot it. Honestly.
I mean, you've known for how many weeks you would need a ride to the hospital? One would think you could save enough money for cab fare in 40 weeks. But ambulances are free.
This is a nice neighborhood, where kids go to private schools. This call is getting lamer.
Met by a nice, well dressed gentleman who directs us upstairs, to his wife, who is allegedly having contractions. I say allegedly, because I'm not sure if she is having contractions, or simply auditioning for a dying walrus.
She hands my partner a 2 inch, pink binder.
"This is my birthing plan. I want to make sure it gets to the hospital with me."
"Excuse me, what? A what plan?"
"My birthing plan. I want to make sure everything goes the way I want it."
"Was going to the hospital by ambulance part of your birthing plan?" (Hey, I'm just curious.)
"Well, no. That part wasn't in the plan."
The binder doesn't make it with us. We forgot it. Honestly.
Easy? Sure.
"This job is easy." Said the man with his paramedic patch that had been sewn on less than 12 months ago. "I mean, why do people think this job is so complicated?"
"Because it is complicated, that's why" came the reply with the more seasoned, yet not a veteran, paramedic.
"No, it's not. This is easy. I can't believe they pay me to do this job, it's so simple."
"How much time a week do you spend studying?"
"Why would I need to study? I already finished paramedic school and passed National Registry."
"Exactly."
It's scary to think we can trust lives with some of these people.
"Because it is complicated, that's why" came the reply with the more seasoned, yet not a veteran, paramedic.
"No, it's not. This is easy. I can't believe they pay me to do this job, it's so simple."
"How much time a week do you spend studying?"
"Why would I need to study? I already finished paramedic school and passed National Registry."
"Exactly."
It's scary to think we can trust lives with some of these people.
Damned Germans
Took an old guy home the other day. Well, not "home" as in his private residence, but "home" as in his very expensive, clean-smelling senior living facility. This is the kind of place in an affluent neighborhood, that costs $10,000 a month just for a room. Well, a suite, really.
These are fun calls for me. They take me out of the 911 system, and I can relax for a few minutes.
He is somewhat hard of hearing, but really nothing is wrong with him. He certainly doesn't meet Medicare guidelines for non-emergent ambulance transportation. That's not my problem though.
He and I talk. He was married for 63 years, until his wife died recently. He still considers himself married, and still wears his wedding band. He has 4 children, 11 grandchildren, 27 great-grandchildren and 2 great-great-grandchildren. He knows each and every one of their names, where they live, and what they do for a living. He also knows which ones come and visit him, and which ones don't. He says I remind him of one of his grandchildren, and that he likes me.
I tell my partner to drive slower and take the long way.
We talk some more. He tells me his secret to staying married for so long was to smile at his wife and say "I'm sorry" alot. He says he married his best friend, and that they never spent a single night apart. He doesn't tear up, but he is visibly saddened that his bride isn't with him any more. He smiles when he talks about her.
We get to his senior-living facility, and wheel him inside. He is obviously very popular with the staff and residents. Every single person says hello to him. His suite is very nice. He has lots of pictures of his family, and they all are attractive people, with big smiles on their faces.
Slimm and I lower the stretcher, and I help him to his chair. He asks me for a favor; to go to his bar and make him a scotch and water. I like this guy even more now.
I bring him his drink and notice a shadow box on the wall. In this shadow box I notice some military insignia, medals, ribbons and such. I notice a Silver Star, Bronze Star, 2 Purple Hearts, and various other medals and ribbons. I count 18 ribbons in the shadow box. I don't recognize the first one. It's blue, with thin red stripes on the ends, with a smaller white strip between the red and blue. I put that image in the back of my head for Wikipedia later.
I notice his Colonel insignia, and I feel mildly ashamed that I called him "Mister" instead of "Colonel." I prefer to call veterans by their rank. I may not have been born in this country, but I certainly feel admiration and respect for veterans.
"What did you get all this ribbons and medals for?"
"Killing all of those damned Germans."
Damned Germans, indeed, Colonel.
Slimm and I both shake his hand, and he gives a manly, respectful handshake, and makes eye contact, and says "thank you" while he does. We bid him goodbye, and make it back to the ambulance to go in service for the next call.
I pull out my iPhone and look up the ribbon online. It's the Distinguished Service Cross. It is the second-highest decoration, only behind the Medal of Honor. I feel honored to have spent time with a true American hero.
Damned Germans, indeed.
These are fun calls for me. They take me out of the 911 system, and I can relax for a few minutes.
He is somewhat hard of hearing, but really nothing is wrong with him. He certainly doesn't meet Medicare guidelines for non-emergent ambulance transportation. That's not my problem though.
He and I talk. He was married for 63 years, until his wife died recently. He still considers himself married, and still wears his wedding band. He has 4 children, 11 grandchildren, 27 great-grandchildren and 2 great-great-grandchildren. He knows each and every one of their names, where they live, and what they do for a living. He also knows which ones come and visit him, and which ones don't. He says I remind him of one of his grandchildren, and that he likes me.
I tell my partner to drive slower and take the long way.
We talk some more. He tells me his secret to staying married for so long was to smile at his wife and say "I'm sorry" alot. He says he married his best friend, and that they never spent a single night apart. He doesn't tear up, but he is visibly saddened that his bride isn't with him any more. He smiles when he talks about her.
We get to his senior-living facility, and wheel him inside. He is obviously very popular with the staff and residents. Every single person says hello to him. His suite is very nice. He has lots of pictures of his family, and they all are attractive people, with big smiles on their faces.
Slimm and I lower the stretcher, and I help him to his chair. He asks me for a favor; to go to his bar and make him a scotch and water. I like this guy even more now.
I bring him his drink and notice a shadow box on the wall. In this shadow box I notice some military insignia, medals, ribbons and such. I notice a Silver Star, Bronze Star, 2 Purple Hearts, and various other medals and ribbons. I count 18 ribbons in the shadow box. I don't recognize the first one. It's blue, with thin red stripes on the ends, with a smaller white strip between the red and blue. I put that image in the back of my head for Wikipedia later.
I notice his Colonel insignia, and I feel mildly ashamed that I called him "Mister" instead of "Colonel." I prefer to call veterans by their rank. I may not have been born in this country, but I certainly feel admiration and respect for veterans.
"What did you get all this ribbons and medals for?"
"Killing all of those damned Germans."
Damned Germans, indeed, Colonel.
Slimm and I both shake his hand, and he gives a manly, respectful handshake, and makes eye contact, and says "thank you" while he does. We bid him goodbye, and make it back to the ambulance to go in service for the next call.
I pull out my iPhone and look up the ribbon online. It's the Distinguished Service Cross. It is the second-highest decoration, only behind the Medal of Honor. I feel honored to have spent time with a true American hero.
Damned Germans, indeed.
Wednesday, September 14, 2011
ProQA Fail
Partner of the day and I had just finished working an incredibly impossible arrest. 17 defibrillations, and almost a complete drug box used. 17 minutes were spent in the house prior to moving the patient, mainly because the personnel on scene were all waiting for a rhythm change, be it positive or negative. We never got one though. That's a different story.
Seriously, who stays in v-fib for 40 minutes?
So, anyway, we get a non-emergent run dropped on us. These are pretty rare, since I have responded emergency to runny noses, and eye pain. This was for a man who was dizzy, which was also interesting. Usually, if a caller even mentions that someone in the house, or the near vicinity, might even be close to remotely being dizzy, or if they know of someone who has ever been dizzy, then a full response is warranted. A full response being a BLS Engine, an ALS Rescue, and an ALS ambulance. Again, I digress.
Suffice it to say that the call taker must have really thought this call was stupid to call it non-emergency.
So, POD and I drive in to this very nice neighborhood, which isn't rare in this part of the county. The houses probably start in the high 400s, and the house we find is probably nearer to the top of the market in this neighborhood.
We've got a waver!
I love wavers. If we didn't have people jumping up and down screaming at us (as if we can hear them from 800 yards through the rolled-up windows, over the diesel engine, the radio traffic, and our general conversation) I have no idea how we would ever find 123 Main Street.
Except for the numbers on the mailbox.
This is a nice looking gentleman, probably not our patient, since our dispatch information is suggesting a 60ish year old. This guy is probably early 30s.
POD and I decide to take in the monitor and the stretcher. Hey, it's the least we could do, right. This call sounds like utter horseshit, but we might as well grab some equipment. And the computer for a refusal. These people usually just want their blood pressure checked.
The waver walks up to us and begins to talk.
“My father and I got home from the gym about 30 minutes ago, and he's been really dizzy since then.”
Okay, maybe not an utter horseshit call, but it still sounds kinda stupid. Waver has an accent that, coupled with his thick, dark hair and complexion, lead me to believe he is middle eastern. That's about as specific as I can get. I can hear a Yankee from across a parking lot, however.
It's 68 degrees in the well-appointed home. I know this because I immediately felt cold when we walked in the door, and happened to walk past the thermostat, where I saw the 68. Just into the living room was a man, lying on the floor. He didn't look good.
Okay, maybe it's a genuine call. This guy looks sick. You know how white people turn kinda blue? This guy looked kinda like a blue middle-eastern guy. And he was wet.
Like, just got out of the pool wet. Obviously, I have a real patient.
He seems to be awake, but to compound his sickness, his son tells me that he only speaks Farsi. I most vertainly do not speak Farsi. I ask all the normal questions for a guy who looks like this.
30 minutes onset after coming home from the gym. No chest pain. No difficulty breathing. No nausea. No vomiting. No syncope. Had a stent placed in Iran 7 years ago. No meds. No allergies. Yada, yada, yada.
All this is going on while I do my best to dry off this incredibly diaphoretic, hirsute man, and get the electrodes to stick to him. Times like this I wish I carried tincture of benzoin in the monitor bag. B/P cycles 72/43.
Well, no wonder I couldn't feel a radial pulse.
The monitor is on, and prints it's initial rhythm strip:
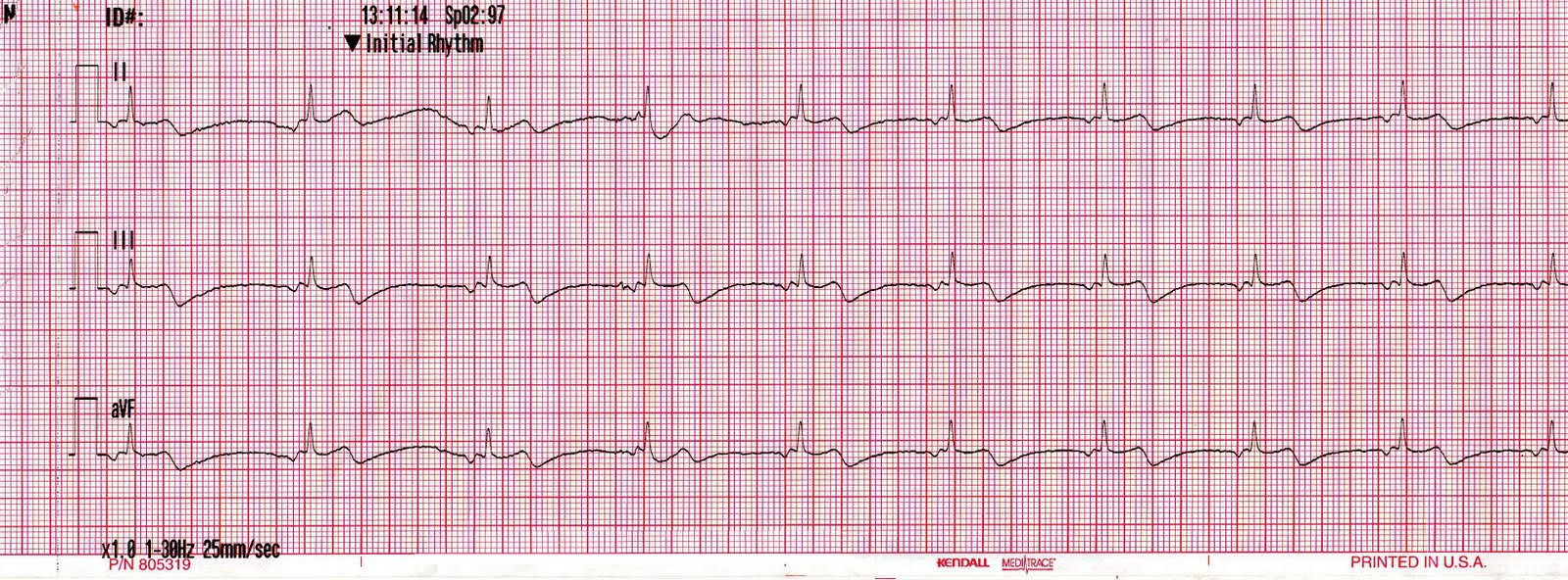
Oh, snap! I would be dizzy too if my heart rate was in the 40s. And if it was junctional.
“Can you tell your father I need to shave some of the hair on his skin, and put more stickers on his chest? Mmmkay, thanks.”
The monitor keeps saying something about “Noisy data.” Forget that, print a damned 12-lead.

Okay, time to go. I reach for the combo pads, just in case this goes south, and also because of a lesson taught to me a long time ago by a coworker.
My Farsi-speaking patient now has eyes the size of dinner plates. His eyes look like he knows I am about to "light him up" or something. He looks at his son and says something incomprehensible to me, and his son in turn looks at me.
“Can you tell me what is going on with my father?”
“He's having a heart attack.”
Surprisingly calm. “Okay. Can we go to Secular Hospital (with no PCI, and notorious for screwing stuff up).
Surprisingly calm. “Okay. Can we go to Secular Hospital (with no PCI, and notorious for screwing stuff up).
“No, but we can go to Saint Catholic, right down the street.” (World-renowned, PCI-capable, and will actually listen to a paramedic and activate the cath lab on our word.) Thankfully, son agrees. As if he had a choice. I am NOT going back in to CQI to explain myself.
POD gives me a nice, smooth ride, which takes about 15 minutes. I get a 16 in an AC somehow, and give him a good, hefty fluid bolus. 324 of aspirin is in. Blood pressure comes up a few points, to 90 systolic. Hey, it's better, but nothing to be too excited about. Thankfully, my service transmits 12-leads, and Saint Catholic felt like answering the phone.
Not only that, they actually hand the phone to not just a physician, but the interventional cardiologist who is awaiting my arrival. I literally transmitted this 12-lead 5 minutes ago, and there is a PCI doc waiting on me?
Cool.
The rest of the story is pretty boring. He went to the cath lab, he got stented, spent the night, then went back home to his son's house. I'd like to check on him, but I probably won't. There's lots of patient's I would like to check on, but I never do.
Sometimes, I start an IV and not much else.
Good call, even with the interesting mistake between 911 call and the actual dispatch. I'm not a dispatcher, but I wonder how something like that happens.
Moving soon.
So I figured out the domain thing. Soon, I will be hosted by EMSblogs, and my blog will be posted on my own website, Captainchairconfessions.
A big thanks to Dave over at EMSblogs.com for his patience in helping me set up my blog. I'm pretty stoked to increase my readership, and to see where this may take me.
I'm also thankful to my readers for making this possible. Especially my friend, Flash Larry. But more on him later.
A big thanks to Dave over at EMSblogs.com for his patience in helping me set up my blog. I'm pretty stoked to increase my readership, and to see where this may take me.
I'm also thankful to my readers for making this possible. Especially my friend, Flash Larry. But more on him later.
So much for social networking.
This social networking thing has gotten out of hand. I have previously commented on one of them, here. I have become quite disappointed in the childish behavior exhibited by my coworkers and colleagues. I seriously thought higher of people than I should have.
One would think, with the seriousness of this profession, there would be a modicum of adult behavior, but no, some of us have decided to resort to name-calling and trash-talking. This is supposed to be a field of adults, but we too often stoop to a high-school level with our behavior. I have been guilty of it as well. But not any more.
So I cleaned up my Facebook friends. No longer will I be "friends" with my coworkers, because, frankly, my coworkers aren't my "friends." They are my "coworkers." I may make a CCC Facebook page later, in an effort to expand my readership, but we will have to see.
I know that several of my readers are my friends on Facebook, and I frankly trust them to maintain my anonymity, and to behave like the adults that I know they are. So, if you are here, and you are there, then I consider you a friend, and I am glad to have you in my life.
One would think, with the seriousness of this profession, there would be a modicum of adult behavior, but no, some of us have decided to resort to name-calling and trash-talking. This is supposed to be a field of adults, but we too often stoop to a high-school level with our behavior. I have been guilty of it as well. But not any more.
So I cleaned up my Facebook friends. No longer will I be "friends" with my coworkers, because, frankly, my coworkers aren't my "friends." They are my "coworkers." I may make a CCC Facebook page later, in an effort to expand my readership, but we will have to see.
I know that several of my readers are my friends on Facebook, and I frankly trust them to maintain my anonymity, and to behave like the adults that I know they are. So, if you are here, and you are there, then I consider you a friend, and I am glad to have you in my life.
Tuesday, September 13, 2011
Excited
I'm getting pretty excited, and anxious. Not teenage-girl-just-broke-up-with-her-soulmate-and-now-wants-to-die anxious, but just mildly anxious.
Dave over at EMSblogs.com has agreed to add my blog to his site. There are some pretty cool blogs over there. 2 of my favorites are TOTWTOTR and Rogue Medic. The others are all good as well. I am excited over becoming a member of a group of excellent writers. I'm anxious over how many people are going to be reading my posts. My friend the historian/organist (I still haven't figured out a nickname for him yet...) will help me through the anxiety.
So, hopefully it happens soon. As soon as I figure out how to change the domain stuff around.
Plus, I'm going to play golf today.
FORE!
Dave over at EMSblogs.com has agreed to add my blog to his site. There are some pretty cool blogs over there. 2 of my favorites are TOTWTOTR and Rogue Medic. The others are all good as well. I am excited over becoming a member of a group of excellent writers. I'm anxious over how many people are going to be reading my posts. My friend the historian/organist (I still haven't figured out a nickname for him yet...) will help me through the anxiety.
So, hopefully it happens soon. As soon as I figure out how to change the domain stuff around.
Plus, I'm going to play golf today.
FORE!
Sunday, September 11, 2011
3,650
That's a lot of days. Or not a lot of days, depending on how you look at it. It's only 10 years.
I have avoided all discussion of today's significance. I mean, really, why must I be reminded to remember something I can never forget?
441 of those were first responders. Firefighters, Police Officers, EMTs and Paramedics.
It was a long time ago, yet it was yesterday.
Everyone, everyone knows where they were that day. Ask anyone born before 1959 where they were on that November day in 1963 when Jack was killed in Dallas. My mother was in Economics class.
I know where I was, and I vividly remember the following 9 days.
If you don't know where I was, it's because I won't discuss it. Some things are better left unsaid.
And that's all I have to say about that.
I have avoided all discussion of today's significance. I mean, really, why must I be reminded to remember something I can never forget?
441 of those were first responders. Firefighters, Police Officers, EMTs and Paramedics.
It was a long time ago, yet it was yesterday.
Everyone, everyone knows where they were that day. Ask anyone born before 1959 where they were on that November day in 1963 when Jack was killed in Dallas. My mother was in Economics class.
I know where I was, and I vividly remember the following 9 days.
If you don't know where I was, it's because I won't discuss it. Some things are better left unsaid.
And that's all I have to say about that.
6:1 is a pretty good ratio.
Accident with possible injuries with airbag deployment 2 miles away.
Whatever.
Slimm is away playing soldier this weekend, and I have partner of the day. It's okay, though. Even though he is an incredible idiot, he follows direction well, like "right" and "left" and "straight."
It's not too far away, and happens to be on the road we are currently on. We would run into the wreck even if we didn't want to.
2 cars, both with front end damage, both facing the same direction. How does that happen? Damage isn't too bad. And, low and behold, there is actually airbag deployment.
As we drive by, and park in a safe spot, I count 9 people standing around doing nothing. 9 people. 2 cars. Seriously?
"Who is driving which car?"
"Uh. This guy is driving the white car, and the girl in the back of the black car was driving the blue car."
Okay. Wait. What? Whatever. I'm on my way to the black car when I feel a tap on my shoulder.
"Hey, what took you guys so long? We have been waiting 20 minutes. And where are the police officers?"
"Which car were you driving, sir?"
"Oh, I wasn't involved in the accident, I just witnessed it happen."
"Okay then. Have a nice day."
Finally I get to the girl in the back seat of the car. Initial impression: not a damned thing wrong with her. And mildly cute.
Before I can open my mouth, someone pipes up. A new person who I hadn't noticed on scene. Oh, that's because she took it upon herself to stop at an accident with bullshit damage and jump all up in my scene. I don't like her before he gets the first syllable out of her mouth.
"Are there any children involved? Because I'm a pediatric nurse, and I can, you know, help out if you need any help. If there are any children."
Well, fantastic. I'm a 9 handicap. Why don't you go grab my 6iron so I can hit make this approach shot?
"No, there aren't any kids involved, but thanks." But maybe you want to hang out in case someone needs their MMR booster.
Finally, I make it to the cute girl. I mean patient. I can clearly see the abrasions on her face from the airbags. Nothing more than superficial. I think she will make it.
"Hi, are you hurting anywhere?"
"No, I told that man not to call for an ambulance. We just need the police department."
"Okay then. Homey is going to take your blood pressure. Can you sign here please?"
"Who are all these people?"
I have no clue, young lady. No clue. As we get in the ambulance to leave the dramatic scene, I spot an additional 3 people getting out of a car across the street and walking towards the crash.
2 cars. 2 drivers. No complaints. 12 bystanders. Not much more bothers me than people who decide to insert themselves into my scene when they know they don't belong.
12 ******* bystanders.
Whatever.
Slimm is away playing soldier this weekend, and I have partner of the day. It's okay, though. Even though he is an incredible idiot, he follows direction well, like "right" and "left" and "straight."
It's not too far away, and happens to be on the road we are currently on. We would run into the wreck even if we didn't want to.
2 cars, both with front end damage, both facing the same direction. How does that happen? Damage isn't too bad. And, low and behold, there is actually airbag deployment.
As we drive by, and park in a safe spot, I count 9 people standing around doing nothing. 9 people. 2 cars. Seriously?
"Who is driving which car?"
"Uh. This guy is driving the white car, and the girl in the back of the black car was driving the blue car."
Okay. Wait. What? Whatever. I'm on my way to the black car when I feel a tap on my shoulder.
"Hey, what took you guys so long? We have been waiting 20 minutes. And where are the police officers?"
"Which car were you driving, sir?"
"Oh, I wasn't involved in the accident, I just witnessed it happen."
"Okay then. Have a nice day."
Finally I get to the girl in the back seat of the car. Initial impression: not a damned thing wrong with her. And mildly cute.
Before I can open my mouth, someone pipes up. A new person who I hadn't noticed on scene. Oh, that's because she took it upon herself to stop at an accident with bullshit damage and jump all up in my scene. I don't like her before he gets the first syllable out of her mouth.
"Are there any children involved? Because I'm a pediatric nurse, and I can, you know, help out if you need any help. If there are any children."
Well, fantastic. I'm a 9 handicap. Why don't you go grab my 6iron so I can hit make this approach shot?
"No, there aren't any kids involved, but thanks." But maybe you want to hang out in case someone needs their MMR booster.
Finally, I make it to the cute girl. I mean patient. I can clearly see the abrasions on her face from the airbags. Nothing more than superficial. I think she will make it.
"Hi, are you hurting anywhere?"
"No, I told that man not to call for an ambulance. We just need the police department."
"Okay then. Homey is going to take your blood pressure. Can you sign here please?"
"Who are all these people?"
I have no clue, young lady. No clue. As we get in the ambulance to leave the dramatic scene, I spot an additional 3 people getting out of a car across the street and walking towards the crash.
2 cars. 2 drivers. No complaints. 12 bystanders. Not much more bothers me than people who decide to insert themselves into my scene when they know they don't belong.
12 ******* bystanders.
Saturday, September 10, 2011
Have you seen this cat?
Missing: Approximately 12 year old, 11 pound, Siamese male cat. Answers to "Buttercup" or "Lorenzo"
Buttercup's owner is currently admitted to local hospital, and cat may be lost and in need of assistance.
Use caution when approaching the cat, as he is known to be very neurotic at times, especially when separated from his neurotic owner for extended periods of time. When communicating with Buttercup, it is best to use an inside, high pitched, baby-talk voice. It is very important that you explain every single movement to Buttercup, lest he suffer a feline psychotic break.
Buttercup may be in need of medical attention, and has been known to crave antifreeze when left home alone without his owner.
If found, Buttercup is easily soothed by large numbers of QVC boxes, bolts of fabric, and Peter Popoff marathons.
He might just need a normal owner.
Buttercup's owner is currently admitted to local hospital, and cat may be lost and in need of assistance.
Use caution when approaching the cat, as he is known to be very neurotic at times, especially when separated from his neurotic owner for extended periods of time. When communicating with Buttercup, it is best to use an inside, high pitched, baby-talk voice. It is very important that you explain every single movement to Buttercup, lest he suffer a feline psychotic break.
Buttercup may be in need of medical attention, and has been known to crave antifreeze when left home alone without his owner.
If found, Buttercup is easily soothed by large numbers of QVC boxes, bolts of fabric, and Peter Popoff marathons.
He might just need a normal owner.
Friday, September 9, 2011
Healthcare is broken
Of course it is. It has been for years. And it will only get worse. Ask Canadians why they come to America to pay cash for their operations instead of sitting on a waiting list.
Today, I transported a man, who called 911 because he was having "burning while urinating." Now, one might opine that perhaps this was a man who had no access to health care, or couldn't afford it, or blah, blah blah. None of that is the case.
This guy lives in an active adult living complex which costs somewhere in the neighborhood of $1,000 per month. His apartment was well-furnished, and I noticed a degree from a 4-year university. His keys had a (what appeared to be fairly new) remote keyless entry for a Buick. He used his iPhone to call his daughter to tell her he would need a ride home from the hospital. He had prescription medications from a private physician. He was well-dressed, in brand-name clothing. Along with his prescription medications, he handed Slimm a Medicare card.
This patient phoned his private physician who informed him that he was unable to make an appointment for today, and suggested the patient seek care in an emergency room. The patient decided that it would be more convenient to call 911, then to get in his own car and drive himself there. He mentioned he wanted to "be seen quicker."
Several thoughts:
This man's problem (likely) could have been treated with a $60 visit to his primary care physician, and with $10 generic antibiotics. Instead, he tied up a valuable resource for 45 minutes, costing Medicare roughly $800 for the ambulance ride, and probably somewhere near $1,500 for the ER visit.
Means testing has been suggested for Social Security. Perhaps it is time to means test Medicare, along with Medicaid. I'm not suggesting that we throw our senior citizens to the wolves. We certainly owe them a debt. But $2,300 for a urinary tract infection?
While healthcare is certainly broken, and in need of fixing, President Obama's suggestion of a single-payor system will never fix the problem, but will only add to the fraud and rampant fiscal irresponsibility. I would propose my idea for a healthcare solution, but that is a topic for another post. I will go so far as to say that a single-payor system will only lead to rationing and a decrease in the quality of care. (See my earlier comment on Canada.)
Shame on the private physician for suggesting the the patient increase the burden on an already over-burdened ER instead of either a) squeezing the patient into the schedule, even if it meant staying late, or b) calling a prescription in to a local pharmacy for an antibiotic, and making an appointment for tomorrow.
Shame on the patient for being so incredibly selfish as to demand a crew of two people, capable of performing meaningful interventions, be taken away from the citizens in their zone to provide him a courtesy ride to the local hospital.
Shame on me for contributing to the fleecing of America.
I would apologize, but if I didn't transport this man to the hospital, then I wouldn't have a job. And my family likes to eat.
(sorry, America)
Today, I transported a man, who called 911 because he was having "burning while urinating." Now, one might opine that perhaps this was a man who had no access to health care, or couldn't afford it, or blah, blah blah. None of that is the case.
This guy lives in an active adult living complex which costs somewhere in the neighborhood of $1,000 per month. His apartment was well-furnished, and I noticed a degree from a 4-year university. His keys had a (what appeared to be fairly new) remote keyless entry for a Buick. He used his iPhone to call his daughter to tell her he would need a ride home from the hospital. He had prescription medications from a private physician. He was well-dressed, in brand-name clothing. Along with his prescription medications, he handed Slimm a Medicare card.
This patient phoned his private physician who informed him that he was unable to make an appointment for today, and suggested the patient seek care in an emergency room. The patient decided that it would be more convenient to call 911, then to get in his own car and drive himself there. He mentioned he wanted to "be seen quicker."
Several thoughts:
This man's problem (likely) could have been treated with a $60 visit to his primary care physician, and with $10 generic antibiotics. Instead, he tied up a valuable resource for 45 minutes, costing Medicare roughly $800 for the ambulance ride, and probably somewhere near $1,500 for the ER visit.
Means testing has been suggested for Social Security. Perhaps it is time to means test Medicare, along with Medicaid. I'm not suggesting that we throw our senior citizens to the wolves. We certainly owe them a debt. But $2,300 for a urinary tract infection?
While healthcare is certainly broken, and in need of fixing, President Obama's suggestion of a single-payor system will never fix the problem, but will only add to the fraud and rampant fiscal irresponsibility. I would propose my idea for a healthcare solution, but that is a topic for another post. I will go so far as to say that a single-payor system will only lead to rationing and a decrease in the quality of care. (See my earlier comment on Canada.)
Shame on the private physician for suggesting the the patient increase the burden on an already over-burdened ER instead of either a) squeezing the patient into the schedule, even if it meant staying late, or b) calling a prescription in to a local pharmacy for an antibiotic, and making an appointment for tomorrow.
Shame on the patient for being so incredibly selfish as to demand a crew of two people, capable of performing meaningful interventions, be taken away from the citizens in their zone to provide him a courtesy ride to the local hospital.
Shame on me for contributing to the fleecing of America.
I would apologize, but if I didn't transport this man to the hospital, then I wouldn't have a job. And my family likes to eat.
(sorry, America)
Thursday, September 8, 2011
On criticism
Recently, a co-worker of mine responded to an accident with possible injuries, which blossomed into an MCI with 4 patients, with 2 possibly critical. While I wasn't there, and won't comment on the assessment or treatment of any of the patients, it's what happened after the call which is interesting.
One of the supposed (and I use the word "supposed" because there seems to be some debate about the actual status of the patient) critical patients, was a young female adult, with left-sided abdominal pain, and a mechanism which lead to a high index of suspicion for a bleeding spleen.
The first medic on scene reportedly (by all parties involved) had two patients immobilized onto long backboards when the second crew arrived. The point of contention seems to be what happened next.
Instead of the second unit leaving rapidly, the crew members elected to remain on scene for (at least) an additional 8 minutes prior to departing to the hospital. They performed a thorough assessment, and attempted IV access twice, without success. The medic member of the crew did not suspect a lacerated or bleeding spleen. While I do not know that particular medic very well, there is nothing I have seen for me to even remotely question his assessments.
The first medic then subsequently immobilized two more patients, and departed for the hospital, arriving prior to the second unit. When questioned about what "took so long" to get to the hospital, the EMT member of the second crew stated "we were doing a thorough assessment and trying for IVs."
Instead of objectively stating the findings of his detailed assessment, the EMT with 18 months of experience told the medic with 18 years to "mind your own business."
One caveat here. I fully believe in the assessment powers of my coworkers. I have worked with many of them, and would freely put my life, or the life of my loved ones in their hands. I always try to avoid criticizing the treatments or interventions performed by others.
About 12 hours later, the EMT decided to insinuate on a social networking site that the first medic on scene was behaving in a "the sky is falling" manner. This led to a long thread of comments, from no fewer than 6 people, on the merits of the call. None of the interventions were called into question. What was called into question was the professionalism of gossip.
I could go on, but won't. Mostly because this is not the place for such a discussion, and partly out of respect to all parties involved, in an effort to minimize the gossip and negative comments.
What I have learned from events surrounding this call:
1. When approached by a colleague, regardless of certification level, or experience, it's always best to listen with objective ears, in an effort to learn something.
2. Discussing a coworker behind their back, whether good, or bad, will always result in that employee finding out what you have said. This is a small community, as referenced in my state, which has been licensing paramedics for 35+ years, with only 12,000 or so reaching certification, with a population approaching 10 million.
3. If you are going to talk about a coworker behind their back, there must be a willingness to accept the ramifications of your actions.
4. Everyone respects the patch, and everyone needs to respect the person wearing the patch.
5. Social networking sites may not be the best place for work-related discussions.
6. Just because it says "Paramedic" on my patch doesn't mean that I can't learn from an EMT.
I have not lost any respect for either one of my coworkers, but have learned an invaluable lesson regarding my professional relationships.
One of the supposed (and I use the word "supposed" because there seems to be some debate about the actual status of the patient) critical patients, was a young female adult, with left-sided abdominal pain, and a mechanism which lead to a high index of suspicion for a bleeding spleen.
The first medic on scene reportedly (by all parties involved) had two patients immobilized onto long backboards when the second crew arrived. The point of contention seems to be what happened next.
Instead of the second unit leaving rapidly, the crew members elected to remain on scene for (at least) an additional 8 minutes prior to departing to the hospital. They performed a thorough assessment, and attempted IV access twice, without success. The medic member of the crew did not suspect a lacerated or bleeding spleen. While I do not know that particular medic very well, there is nothing I have seen for me to even remotely question his assessments.
The first medic then subsequently immobilized two more patients, and departed for the hospital, arriving prior to the second unit. When questioned about what "took so long" to get to the hospital, the EMT member of the second crew stated "we were doing a thorough assessment and trying for IVs."
Instead of objectively stating the findings of his detailed assessment, the EMT with 18 months of experience told the medic with 18 years to "mind your own business."
One caveat here. I fully believe in the assessment powers of my coworkers. I have worked with many of them, and would freely put my life, or the life of my loved ones in their hands. I always try to avoid criticizing the treatments or interventions performed by others.
About 12 hours later, the EMT decided to insinuate on a social networking site that the first medic on scene was behaving in a "the sky is falling" manner. This led to a long thread of comments, from no fewer than 6 people, on the merits of the call. None of the interventions were called into question. What was called into question was the professionalism of gossip.
I could go on, but won't. Mostly because this is not the place for such a discussion, and partly out of respect to all parties involved, in an effort to minimize the gossip and negative comments.
What I have learned from events surrounding this call:
1. When approached by a colleague, regardless of certification level, or experience, it's always best to listen with objective ears, in an effort to learn something.
2. Discussing a coworker behind their back, whether good, or bad, will always result in that employee finding out what you have said. This is a small community, as referenced in my state, which has been licensing paramedics for 35+ years, with only 12,000 or so reaching certification, with a population approaching 10 million.
3. If you are going to talk about a coworker behind their back, there must be a willingness to accept the ramifications of your actions.
4. Everyone respects the patch, and everyone needs to respect the person wearing the patch.
5. Social networking sites may not be the best place for work-related discussions.
6. Just because it says "Paramedic" on my patch doesn't mean that I can't learn from an EMT.
I have not lost any respect for either one of my coworkers, but have learned an invaluable lesson regarding my professional relationships.
Baba O'Riley
Riding through the city, with my iPod playing, and The Who comes on. I didn't plan on The Who, as I normally have to be in the "mood" for their music. I won't argue their artistic talents with anyone, just not my normal taste.
Baba O'Riley.
Or, as the uninitiated call it, "Teenage Wasteland."
This song reminds me of one of my favorite partners, who, because of this song, I now refer to as "Sally." I have been graced with some of the best partners anyone could ever have asked for in my career, and was deserving of very few of them. We only spent 9 months together, until the Cajun took my place. I wish it could have been longer.
Our first shift together was at a strange transition. I had just finished three months of critical care training, third rides and monumental amounts of studying, along with a change in shifts from a day truck, back to nights.
"Hi. Are you going to be my new partner?"
"Hurrrumphff. I don't know."
"Well, I'm excited."
"Mmmmmmhmmmm."
Fifteen minutes of silence as we drove to our posting location for the evening in a fine, upstanding neighborhood full of food stamps and illegal aliens.
"Hey, do you want some Gouda?"
"Some what?"
"Gouda. You know, cheese. And crackers?"
"Seriously?" (I mean, who seriously brings Gouda and crackers to work on an ambulance?)
"Sure. Thanks."
We turned out to work fantastically together. We shared lots in common. We both have a child around the same age. We shared many nights of Handel on the Law podcasts, and yelling at dispatchers. We shared watermelon gum and hunts for clean bathrooms. She reaffirmed my love for iced coffee. We lived close to each other. She introduced me to some interesting and new beer, and I introduced her to limoncello. (Off duty, of course.) We shared a mutual hatred for people who abuse the 911 system, and the nurses who were of a below-average intellect who we turned over said people to. We shared many evenings watching the patrons of the local immigrant club, and enjoyed the transvestite Thursdays. And she brought good food to work, and always shared.
She told me the stories of moving to the west coast for the forests and hiking. And how she had to move back because she ran out of money. She is, and was, the ideal partner. I look forward to the chance meetings we have, as we now work opposite rotations, she at night, and me during the day. I like hearing her call me "Big Daddy." And I miss working with her.
"Sally take my hand. We'll travel south cross land."
The Cajun had better take care of her.
Baba O'Riley.
Or, as the uninitiated call it, "Teenage Wasteland."
This song reminds me of one of my favorite partners, who, because of this song, I now refer to as "Sally." I have been graced with some of the best partners anyone could ever have asked for in my career, and was deserving of very few of them. We only spent 9 months together, until the Cajun took my place. I wish it could have been longer.
Our first shift together was at a strange transition. I had just finished three months of critical care training, third rides and monumental amounts of studying, along with a change in shifts from a day truck, back to nights.
"Hi. Are you going to be my new partner?"
"Hurrrumphff. I don't know."
"Well, I'm excited."
"Mmmmmmhmmmm."
Fifteen minutes of silence as we drove to our posting location for the evening in a fine, upstanding neighborhood full of food stamps and illegal aliens.
"Hey, do you want some Gouda?"
"Some what?"
"Gouda. You know, cheese. And crackers?"
"Seriously?" (I mean, who seriously brings Gouda and crackers to work on an ambulance?)
"Sure. Thanks."
We turned out to work fantastically together. We shared lots in common. We both have a child around the same age. We shared many nights of Handel on the Law podcasts, and yelling at dispatchers. We shared watermelon gum and hunts for clean bathrooms. She reaffirmed my love for iced coffee. We lived close to each other. She introduced me to some interesting and new beer, and I introduced her to limoncello. (Off duty, of course.) We shared a mutual hatred for people who abuse the 911 system, and the nurses who were of a below-average intellect who we turned over said people to. We shared many evenings watching the patrons of the local immigrant club, and enjoyed the transvestite Thursdays. And she brought good food to work, and always shared.
She told me the stories of moving to the west coast for the forests and hiking. And how she had to move back because she ran out of money. She is, and was, the ideal partner. I look forward to the chance meetings we have, as we now work opposite rotations, she at night, and me during the day. I like hearing her call me "Big Daddy." And I miss working with her.
"Sally take my hand. We'll travel south cross land."
The Cajun had better take care of her.
Tuesday, September 6, 2011
Don't stop, don't call
"Medic Sixtynine, respond to reports of an accident with possible injuries, Goofball Highway at Old Booger Hill Road. Passerby advises there are 4 cars involved, unsure of any injuries."
Great. This call sounds F-U-N. And it's raining. And Old Booger Hill Road crosses Goofball Highway at least 4 separate times within 6 miles. In two distinct fire districts, covered by three different engine companies.
Lets run down why this call sucks:
1. Day after a holiday, at 8:30am.
2. In the rain
3. An unknown location
4. Some cellphone warrior was worried enough to call, but not enough to stop, and actually roll down the damned window and shout "Hey, y'all'rite?"
5. I haven't had my breakfast yet
6. I haven't had my nap yet
7 I haven't even put on my socks yet
We literally drive in circles looking for this wreck. This cellphone warrior was kind enough to call 911, but couldn't give a description of the cars. Fan-freaking-tastic.
We find a wreck. A red SUV and a white Ram Truck.
Not the wreck. Fire says it "uppathattaway" about half a mile.
Dark SUV, grey BMW, white sedan.
Wrong wreck. Turn around again, check another intersection of Goofball Highway and Old Booger Hill.
Find a wreck. PD is on scene. Eating a biscuit in his car. (I am NOT kidding.)
"Hey, where y'all been? We been waitin' on y'all for a while now."
"Shut up, Munch*. Who's hurt?"
"Oh, ain't nobody hurt. I done cancelled y'all 'bout five minutes ago."
I hate cellphone warriors. And missing breakfast.
I put my socks on, and go in service.
Great. This call sounds F-U-N. And it's raining. And Old Booger Hill Road crosses Goofball Highway at least 4 separate times within 6 miles. In two distinct fire districts, covered by three different engine companies.
Lets run down why this call sucks:
1. Day after a holiday, at 8:30am.
2. In the rain
3. An unknown location
4. Some cellphone warrior was worried enough to call, but not enough to stop, and actually roll down the damned window and shout "Hey, y'all'rite?"
5. I haven't had my breakfast yet
6. I haven't had my nap yet
7 I haven't even put on my socks yet
We literally drive in circles looking for this wreck. This cellphone warrior was kind enough to call 911, but couldn't give a description of the cars. Fan-freaking-tastic.
We find a wreck. A red SUV and a white Ram Truck.
Not the wreck. Fire says it "uppathattaway" about half a mile.
Dark SUV, grey BMW, white sedan.
Wrong wreck. Turn around again, check another intersection of Goofball Highway and Old Booger Hill.
Find a wreck. PD is on scene. Eating a biscuit in his car. (I am NOT kidding.)
"Hey, where y'all been? We been waitin' on y'all for a while now."
"Shut up, Munch*. Who's hurt?"
"Oh, ain't nobody hurt. I done cancelled y'all 'bout five minutes ago."
I hate cellphone warriors. And missing breakfast.
I put my socks on, and go in service.
Take the bag!
My service has a policy which requires the crew to take in the stretcher, cardiac monitor, and jump bag to every patient. I have been in the habit of taking said equipment in, even without a written policy.
While taking a cardiac monitor in to a 10 year old with a twisted ankle may be a little over kill, that's what the bosses want, so we do it. Or at least I do.
It's also a good practice. Seriously, what are you going to do for a patient who accidentally stabbed himself in the femoral artery with a turkey baster right before Thanksgiving dinner, and now there is blood squirting every which way, in the squash casserole, and all over the turkey, and the mashed potatoes, and your jump bag is 30 yards away in the ambulance? And when that call happens (and we all know it will happen, to someone), you just know there is going to be a doctor/nurse/paramedic/personal-injury lawyer watching your big, fat, screw-up.
"Ma'am, can I borrow a towel from you since I'm too lazy to bring in my equipment?"
Take in the damned bag. Take in the damned monitor. Put it on the effing stretcher so your lazy ass doesn't hurt your lazy back carrying it.
I hate lazy people.
While taking a cardiac monitor in to a 10 year old with a twisted ankle may be a little over kill, that's what the bosses want, so we do it. Or at least I do.
It's also a good practice. Seriously, what are you going to do for a patient who accidentally stabbed himself in the femoral artery with a turkey baster right before Thanksgiving dinner, and now there is blood squirting every which way, in the squash casserole, and all over the turkey, and the mashed potatoes, and your jump bag is 30 yards away in the ambulance? And when that call happens (and we all know it will happen, to someone), you just know there is going to be a doctor/nurse/paramedic/personal-injury lawyer watching your big, fat, screw-up.
"Ma'am, can I borrow a towel from you since I'm too lazy to bring in my equipment?"
Take in the damned bag. Take in the damned monitor. Put it on the effing stretcher so your lazy ass doesn't hurt your lazy back carrying it.
I hate lazy people.
Saturday, September 3, 2011
Good Luck, Cupcake
So tonight is Cupcake's first night on her own as a Paramedic. Tests have been passed, uniforms ordered and received, patches sewn on, third rides complete, and she is being "thrown to the wolves" as they say.
I had the pleasure of working with Cupcake for over a year, and we became good friends. She is one of the best partners I have ever had. She was always there to have my back, and saved me more times than I can count. She is a damned good EMT, and will be a fantastic paramedic.
Good luck, Cupcake.
I had the pleasure of working with Cupcake for over a year, and we became good friends. She is one of the best partners I have ever had. She was always there to have my back, and saved me more times than I can count. She is a damned good EMT, and will be a fantastic paramedic.
Good luck, Cupcake.
Friday, September 2, 2011
Fore!
Not really pertinent to EMS-related stuff, but this is my blog, and frankly, I can post what I want.
I whooped that golf course today. I was 8 over, playing from the tips, which is a personal best for me. I bested my handicap by 4 strokes, and when adjusted, my handicap will be down to 9.8.
I hit 11/14 fairways, and 15 greens in regulation, and stayed out of the hazards all day. A few three-putts, but there were many more good shots than bad. I must be getting good at this. Either that, or today was a terrible fluke, and I really do suck at golf.
I didn't lose a single ball, either.
I whooped that golf course today. I was 8 over, playing from the tips, which is a personal best for me. I bested my handicap by 4 strokes, and when adjusted, my handicap will be down to 9.8.
I hit 11/14 fairways, and 15 greens in regulation, and stayed out of the hazards all day. A few three-putts, but there were many more good shots than bad. I must be getting good at this. Either that, or today was a terrible fluke, and I really do suck at golf.
I didn't lose a single ball, either.
Thursday, September 1, 2011
Impressive
From a patient's H&P: (edited somewhat, of course...)
History significant for :
History significant for :
- Non-insulin-dependent diabetes controlled with diet.
- Hypertension
- Asthma
- Obstructive sleep apnea, requiring CPAP at 18cmH2O (WOW!)
- Chronic renal failure, requiring hemodialysis
- Cardiomyopathy with ejection fraction of 40%
- Peripheral vascular disease
- Hypercholesterolemia
- Neuropathy
- Acute respiratory failure requiring tracheostomy and mechanical ventilation
- Morbid obesity with a BMI > 60
- Depression (ya think?)
- 15 pack-year smoker, with frequent marijuana abuse
Hey! Didn't I see this house on TV?
I don't care for abdominal pain. They are generally the most lame calls ever. If your tummy hurts so bad that you need to call the ambulance, you had better be close to death if you want any sympathy.
We can't get in this house. Hoarder-style. Smell it from the street. It smells like rotting death covered in trash and human waste. From 40 yards away.
Seriously, I don't know how this house hasn't exploded from the sheer amount of crap stuffed inside of it.
Literally, this guy should be on TV. If you've ever seen Hoarders on A&E, then you have a good frame of reference for just how full of crap this house is.
If you have ever worked on an ambulance, you have a good frame of reference for just how full of crap this guy is.
This guy has abdominal pain (allegedly) that is so bad, he absolutely has to go to the hospital, but, oh, let him get some shoes first, and find a book to take with him. Mom, you can ride up front. I'm impressed with your lack of ability to find clothes that match with all that crap you have in your house. Hey, at least the clothes are clean, and I don't have to turn on the exhaust fan in the back of the ambulance.
Slimm advises me discreetly that Tummyacher just got back from the doctor's office 3 hours ago with pain med prescriptions.
Now he is known as Faketummyacherseeker.
Interestingly enough, I catch him peeking over his shoulder at me. I am, of course, sitting in the Captain chair, from which I frequently write my blog posts. Unless you are my boss, then I write them after I get home, on my own time.
Each time he looks at me (I am generally ignoring him, of course, because, frankly, I think he's full of shit), his whines and whimpers get just a little bit louder.
"What does the pain feel like?"
"Oh, it's awful. I can't really describe it. It hurts really bad."
"How bad on a scale of 1-10?"
"Twelve."
Obviously not a mathematician. "Does anything make it worse?"
"Moving makes it worse. It's just terrible."
"Does anything make it better?"
"Usually Dilaudid makes the pain go away. OOOOhhhhhhh, ithurtsbad!"
Of course it does, Mr. Faketummyacherseeker, of course it does.
We can't get in this house. Hoarder-style. Smell it from the street. It smells like rotting death covered in trash and human waste. From 40 yards away.
Seriously, I don't know how this house hasn't exploded from the sheer amount of crap stuffed inside of it.
Literally, this guy should be on TV. If you've ever seen Hoarders on A&E, then you have a good frame of reference for just how full of crap this house is.
If you have ever worked on an ambulance, you have a good frame of reference for just how full of crap this guy is.
This guy has abdominal pain (allegedly) that is so bad, he absolutely has to go to the hospital, but, oh, let him get some shoes first, and find a book to take with him. Mom, you can ride up front. I'm impressed with your lack of ability to find clothes that match with all that crap you have in your house. Hey, at least the clothes are clean, and I don't have to turn on the exhaust fan in the back of the ambulance.
Slimm advises me discreetly that Tummyacher just got back from the doctor's office 3 hours ago with pain med prescriptions.
Now he is known as Faketummyacherseeker.
Interestingly enough, I catch him peeking over his shoulder at me. I am, of course, sitting in the Captain chair, from which I frequently write my blog posts. Unless you are my boss, then I write them after I get home, on my own time.
Each time he looks at me (I am generally ignoring him, of course, because, frankly, I think he's full of shit), his whines and whimpers get just a little bit louder.
"What does the pain feel like?"
"Oh, it's awful. I can't really describe it. It hurts really bad."
"How bad on a scale of 1-10?"
"Twelve."
Obviously not a mathematician. "Does anything make it worse?"
"Moving makes it worse. It's just terrible."
"Does anything make it better?"
"Usually Dilaudid makes the pain go away. OOOOhhhhhhh, ithurtsbad!"
Of course it does, Mr. Faketummyacherseeker, of course it does.
Monday, August 29, 2011
Non-emergency?
Earlier, I discussed the disproportionate use of lights and sirens in our responses. Sure enough, someone just has to prove me wrong.
We are responding to a doc-in-the-box that calls our service at least once a day. This clinic doesn't have a stellar reputation, nor does it have a terrible reputation. Just another urgent care facility.
Apparently, they called my dispatch center directly and requested an ambulance. Somewhere during that conversation, an employee at said urgent care facility mentioned that the patient was complaining of chest pain. And difficulty breathing. And has a history of PE. And an abnormal EKG.
...And wants us to come non emergency.
This patient was genuinely sick. She was in sinus tach at 130, and in obvious distress. Her room air O2 saturations were very easy to take, as the clinic staff hadn't bothered to administer any, much less check her SpO2. It was 88. The staff did, however, start a 24 gauge INT for me. Sweet.
Her 12-lead, physical exam and history all scream PE. And this doctor either:
A. Didn't know it. (Which makes me wonder why not)
B. Wasn't that concerned about it. (Which makes me want to ask him why) ...or...
C. Knew that I personally would be the one to respond and take care of the patient. (Which makes me want to shake his hand.)
Maybe I'm just complaining too much.
We are responding to a doc-in-the-box that calls our service at least once a day. This clinic doesn't have a stellar reputation, nor does it have a terrible reputation. Just another urgent care facility.
Apparently, they called my dispatch center directly and requested an ambulance. Somewhere during that conversation, an employee at said urgent care facility mentioned that the patient was complaining of chest pain. And difficulty breathing. And has a history of PE. And an abnormal EKG.
...And wants us to come non emergency.
This patient was genuinely sick. She was in sinus tach at 130, and in obvious distress. Her room air O2 saturations were very easy to take, as the clinic staff hadn't bothered to administer any, much less check her SpO2. It was 88. The staff did, however, start a 24 gauge INT for me. Sweet.
Her 12-lead, physical exam and history all scream PE. And this doctor either:
A. Didn't know it. (Which makes me wonder why not)
B. Wasn't that concerned about it. (Which makes me want to ask him why) ...or...
C. Knew that I personally would be the one to respond and take care of the patient. (Which makes me want to shake his hand.)
Maybe I'm just complaining too much.
Sunday, August 28, 2011
Not a happy Hanukkah
It was Christmas season, only a few days before. Actually, it was in the middle of Hanukkah, which is pertinent, given the Star of David around his neck.
It was late evening, when most normal people are winding down, in bed, perhaps with a snack, or watching some late news. The address was for a fairly nice neighborhood, full of upper-middle class homes, and successful people. For a man "not feeling well."
Cupcake and I arrived only a few minutes behind the first-in Engine and Rescue units. We took our stretcher and first-in bag with us into the well-appointed home, and were directed through a
kitchen, full of pictures of children and what appeared to be a new grandchild.
As I rounded the corner, Elrod and I made eye contact, and I saw the distinct look of fear in his eyes. The look that says "this guy is sick something bad." Elrod is a career paramedic, with 20 years under his belt. He has seen some sick people before. His eyes tell me enough. Elrod is starting a line while Tim is hooking up the monitor and Kevin puts a nonrebreather on him. I look at the wife. "What's going on?"
"He hasn't felt good for a few days. He just took the trash out, and came in and said he couldn't breathe."
"No, he doesn't take any medications."
I get a glimpse of the patient in the dim light, with the glow of Fox News in the background. He looks terrible. Like, as my father would say, "death eatin' a cracker." His skin is grey. An amalgamation of pale, cyanotic, diaphoretic and dusky.
"Forget the line, Elrod. Let's get him on the stretcher."
Cupcake and I are out of the house with the patient within 4 minutes of walking in. She asks if I want a rider to the hospital, which is 10 minutes away. 6 minutes with her heavy foot.
"I want to leave. If there is a rider in the back with me when you get up front, so be it. Otherwise, lets get the hell out of here."
No rider.
O2 saturation is 88% with 15 liters going. I get a blood pressure that is terrible. 82/50. His carotid is incredibly fast and weak. The monitor is counting out 140. A minute later I have two 16 gauge lines going. I don't know how I found those veins, but I did. His skin still looks terrible.
I'm throwing the 12-lead on as fast as I possibly can.
"I can't breathe."
"I know, buddy. I can breathe for you if you would like, so you can try and relax."
"Okay."
I drop an NPA in and start bagging him. "Data quality prohibits interpretation" says the monitor. Shit. I don't need a crappy algorithm to tell me this guy had a massive MI over the past few days. B/P cycles again: 73/49.
Cupcake tells me we are 2 minutes away from the hospital. That's two minutes too long. He should have been there 2 days ago.
We unload him from the truck. "I'm about to die."
Cupcake says "no you aren't, there are really good doctors in here, and they are going to take great care of you."
We walk with incredible alacrity into the ER, and the receiving doc sees my NPA, and shows us to a room close by. "Let's get RSI."
"I'm going to put you to sleep and put a tube in your throat so we can breathe for you."
"Okay."
The drugs are in, and the tube follows quickly. As does the noises from the monitor. V-tach. "He have a pulse?" "No." "Start CPR."
Normally, I am out of the room at this point, so the more educated people can do their jobs. Usually, I am just in the way. Not this time. I'm right there. I haven't had time to leave yet, and the crash cart is blocking my exit. I start compressions, pushing hard and fast on this man that was talking to me just moments ago.
Epi is in. Charge. Shock. Asystole.
More compressions. Something catches my eye at the door to the room. It's Cupcake, and she has turned her head. I hear a vaguely familiar, polite voice: "Is he doing better?..." as I see his wife come around the curtain.
We make eye contact and she sees me doing chest compressions on her husband of 30 years.
What followed was the most terrible, shrill, eardrum piercing sound I have ever heard. The sound that all of my fellow EMSers have heard, and dread hearing again. It's the sound that still, to this day, awakens me occasionally from a still sleep.
The next few minutes were a blur. More drugs are pushed, more joules are administered, all with no effect. The wife has since come into the room, and is sitting on a chair next to her husband, talking to him, as I continue to compress his heart, and respiratory continues to inflate his lungs.
"You can't go now, you need to come back. You can't leave me."
"It's okay if you need to go, honey. I understand. You are a wonderful husband."
I can't believe I am seeing these stages of grief happen in front of me. She looks at the doctor.
"I think he's gone. He's not coming back."
Doctor and I make eye contact, and he gives me an almost imperceptible nod. I stop, and walk out the room, then I hear the wife again.
"Wait."
I turn around, and she looks through my eyes, hers full of tears, and mine full of failure.
"You did a great job. I know you took good care of Danny, and you did everything you could. Make sure you go home and hug your wife real good, and kiss that sweet boy of yours."
How on earth did she know I was married, with a young child? Oh, damn, his 3 month picture is on my nametag.
She hugged me hard. For what seemed like an eternity, and I returned to my ambulance with her tears soaking my shirt, and a few of mine on my cheeks.
3 days later I read his obituary. He was a lawyer. His office was only blocks from mine. He was an avid tennis player, and a father of 3, with a baby granddaughter.
I wish he would have called earlier.
It was late evening, when most normal people are winding down, in bed, perhaps with a snack, or watching some late news. The address was for a fairly nice neighborhood, full of upper-middle class homes, and successful people. For a man "not feeling well."
Cupcake and I arrived only a few minutes behind the first-in Engine and Rescue units. We took our stretcher and first-in bag with us into the well-appointed home, and were directed through a
kitchen, full of pictures of children and what appeared to be a new grandchild.
As I rounded the corner, Elrod and I made eye contact, and I saw the distinct look of fear in his eyes. The look that says "this guy is sick something bad." Elrod is a career paramedic, with 20 years under his belt. He has seen some sick people before. His eyes tell me enough. Elrod is starting a line while Tim is hooking up the monitor and Kevin puts a nonrebreather on him. I look at the wife. "What's going on?"
"He hasn't felt good for a few days. He just took the trash out, and came in and said he couldn't breathe."
"No, he doesn't take any medications."
I get a glimpse of the patient in the dim light, with the glow of Fox News in the background. He looks terrible. Like, as my father would say, "death eatin' a cracker." His skin is grey. An amalgamation of pale, cyanotic, diaphoretic and dusky.
"Forget the line, Elrod. Let's get him on the stretcher."
Cupcake and I are out of the house with the patient within 4 minutes of walking in. She asks if I want a rider to the hospital, which is 10 minutes away. 6 minutes with her heavy foot.
"I want to leave. If there is a rider in the back with me when you get up front, so be it. Otherwise, lets get the hell out of here."
No rider.
O2 saturation is 88% with 15 liters going. I get a blood pressure that is terrible. 82/50. His carotid is incredibly fast and weak. The monitor is counting out 140. A minute later I have two 16 gauge lines going. I don't know how I found those veins, but I did. His skin still looks terrible.
I'm throwing the 12-lead on as fast as I possibly can.
"I can't breathe."
"I know, buddy. I can breathe for you if you would like, so you can try and relax."
"Okay."
I drop an NPA in and start bagging him. "Data quality prohibits interpretation" says the monitor. Shit. I don't need a crappy algorithm to tell me this guy had a massive MI over the past few days. B/P cycles again: 73/49.
Cupcake tells me we are 2 minutes away from the hospital. That's two minutes too long. He should have been there 2 days ago.
We unload him from the truck. "I'm about to die."
Cupcake says "no you aren't, there are really good doctors in here, and they are going to take great care of you."
We walk with incredible alacrity into the ER, and the receiving doc sees my NPA, and shows us to a room close by. "Let's get RSI."
"I'm going to put you to sleep and put a tube in your throat so we can breathe for you."
"Okay."
The drugs are in, and the tube follows quickly. As does the noises from the monitor. V-tach. "He have a pulse?" "No." "Start CPR."
Normally, I am out of the room at this point, so the more educated people can do their jobs. Usually, I am just in the way. Not this time. I'm right there. I haven't had time to leave yet, and the crash cart is blocking my exit. I start compressions, pushing hard and fast on this man that was talking to me just moments ago.
Epi is in. Charge. Shock. Asystole.
More compressions. Something catches my eye at the door to the room. It's Cupcake, and she has turned her head. I hear a vaguely familiar, polite voice: "Is he doing better?..." as I see his wife come around the curtain.
We make eye contact and she sees me doing chest compressions on her husband of 30 years.
What followed was the most terrible, shrill, eardrum piercing sound I have ever heard. The sound that all of my fellow EMSers have heard, and dread hearing again. It's the sound that still, to this day, awakens me occasionally from a still sleep.
The next few minutes were a blur. More drugs are pushed, more joules are administered, all with no effect. The wife has since come into the room, and is sitting on a chair next to her husband, talking to him, as I continue to compress his heart, and respiratory continues to inflate his lungs.
"You can't go now, you need to come back. You can't leave me."
"It's okay if you need to go, honey. I understand. You are a wonderful husband."
I can't believe I am seeing these stages of grief happen in front of me. She looks at the doctor.
"I think he's gone. He's not coming back."
Doctor and I make eye contact, and he gives me an almost imperceptible nod. I stop, and walk out the room, then I hear the wife again.
"Wait."
I turn around, and she looks through my eyes, hers full of tears, and mine full of failure.
"You did a great job. I know you took good care of Danny, and you did everything you could. Make sure you go home and hug your wife real good, and kiss that sweet boy of yours."
How on earth did she know I was married, with a young child? Oh, damn, his 3 month picture is on my nametag.
She hugged me hard. For what seemed like an eternity, and I returned to my ambulance with her tears soaking my shirt, and a few of mine on my cheeks.
3 days later I read his obituary. He was a lawyer. His office was only blocks from mine. He was an avid tennis player, and a father of 3, with a baby granddaughter.
I wish he would have called earlier.
You thought texting while driving was bad.
So Slimm and I are awoken from a nap to respond to a man with a piece of a metal fence stuck in his leg.
We were having a good nap. There had better be a humongous piece of metal stuck in this man's leg.
Finally we find the guy. About as far away from the entrance to the scene as you can get. I will, and did, drive my ambulance across a football field, baseball field, and a lacrosse field.
Sure enough, this guy has a piece of a metal fence, the kind used to hold up silk fences around construction sites, impaled in the back of his leg. Well done, man, well done. Thank you for interrupting my nap with a genuine problem.
"How did this happen?"
"I was texting my daughter while walking, and tripped, and fell down. I guess I just landed the right way."
He's gonna be OK. After some surgery, that is.
We were having a good nap. There had better be a humongous piece of metal stuck in this man's leg.
Finally we find the guy. About as far away from the entrance to the scene as you can get. I will, and did, drive my ambulance across a football field, baseball field, and a lacrosse field.
Sure enough, this guy has a piece of a metal fence, the kind used to hold up silk fences around construction sites, impaled in the back of his leg. Well done, man, well done. Thank you for interrupting my nap with a genuine problem.
"How did this happen?"
"I was texting my daughter while walking, and tripped, and fell down. I guess I just landed the right way."
He's gonna be OK. After some surgery, that is.
Pleasant Vomiting
Respond emergency for a female who feels sick, and with a racing heart.
Sounds cool enough. (I like giving adenosine.)
We are met by the fire crew. "Leave your stretcher in the ambulance. She will be sitting on a john boat in the driveway."
Interesting. (What's that bout a john boat?...)
"I vomited violently about an hour ago, and I want to go to the hospital. I laid down, and my heart started racing."
Sinus tach at 113.
"Violent vomiting" was mentioned no fewer than 15 times on the way to the hospital.
Straight to triage.
Sounds cool enough. (I like giving adenosine.)
We are met by the fire crew. "Leave your stretcher in the ambulance. She will be sitting on a john boat in the driveway."
Interesting. (What's that bout a john boat?...)
"I vomited violently about an hour ago, and I want to go to the hospital. I laid down, and my heart started racing."
Sinus tach at 113.
"Violent vomiting" was mentioned no fewer than 15 times on the way to the hospital.
Straight to triage.
Thursday, August 25, 2011
Red lights for this?
We go "emergency" way to much. Period. My unit is dispatched emergency to well over 95% of our calls. I transport emergency to the hospital maybe once a month.
At my service, the dispatchers will raise a unit for a call by saying "Unit soandso, copy an emergency." It seems that every imaginable complaint under the sun is an "emergency." And when we respond emergency, it means that we are going to a scene with some sort of fire apparatus. It's not the dispatcher's fault.
Perhaps we should better educate the public on the definition of "emergency."
Why do we need 6 EMTs and 2 Paramedics in, collectively, a fire engine, rescue truck, and an ambulance for a 35 year old man with kidney stones? Or for that matter, a child with a fever? Or for the nursing home patient with abnormal labs?
Those people need a taxi, not an ambulance, much less 3 humongous vehicles driving emergency, forcing cars to the side of the road for their bullshit complaint.
I think the call-takers in my county should be able to provide directions to the hospital.
At my service, the dispatchers will raise a unit for a call by saying "Unit soandso, copy an emergency." It seems that every imaginable complaint under the sun is an "emergency." And when we respond emergency, it means that we are going to a scene with some sort of fire apparatus. It's not the dispatcher's fault.
Perhaps we should better educate the public on the definition of "emergency."
Why do we need 6 EMTs and 2 Paramedics in, collectively, a fire engine, rescue truck, and an ambulance for a 35 year old man with kidney stones? Or for that matter, a child with a fever? Or for the nursing home patient with abnormal labs?
Those people need a taxi, not an ambulance, much less 3 humongous vehicles driving emergency, forcing cars to the side of the road for their bullshit complaint.
I think the call-takers in my county should be able to provide directions to the hospital.
Wednesday, August 24, 2011
You can downgrade now.
A call for an infection in the leg. Bullshit.
Not only does this guy have maggots in the open wounds on both legs, but he appears to have been incontinent for several days. DAYS. Literally, covered in shit. The rest of the assessment is unremarkable, with normal vitals.
I know it stinks, and you can smell it up front, but there's not really reason for you to drive emergency to the hospital.
Not only does this guy have maggots in the open wounds on both legs, but he appears to have been incontinent for several days. DAYS. Literally, covered in shit. The rest of the assessment is unremarkable, with normal vitals.
I know it stinks, and you can smell it up front, but there's not really reason for you to drive emergency to the hospital.
Tuesday, August 23, 2011
I like my partner.
I have spent the better part of the past three years working with members of the opposite sex. It seems to work out well for my company, and that's cool with me. We seem to do lots of female psych calls. I mean LOTS. It might be something in the water.
I've had only good partners lately. Well, except for the occasional McTalkalot and McAsksalotofquestions, and Dragon Breath. But whatever.
Recently, I was assigned a new partner, Slimm. This is Slimm's first ALS 911 ambulance. He has some good experience on a non-emergency truck, and a good head on his shoulders. He has been learning how to run 12-leads, set up ventilators, and has gotten some good interventions under his belt. He is going to be a fantastic paramedic one day. We get along well, and our personalities mesh well together. I like to run scenes quickly, and move patients to the ambulance, so the fire crews can go back in service and get back to their games of checkers. Slimm just wants to take people to the hospital.
Slimm laughs at my jokes, too. Which helps.
Plus, he drives as smooth as butter. It will be a sad day when Slimm gets moved.
I've had only good partners lately. Well, except for the occasional McTalkalot and McAsksalotofquestions, and Dragon Breath. But whatever.
Recently, I was assigned a new partner, Slimm. This is Slimm's first ALS 911 ambulance. He has some good experience on a non-emergency truck, and a good head on his shoulders. He has been learning how to run 12-leads, set up ventilators, and has gotten some good interventions under his belt. He is going to be a fantastic paramedic one day. We get along well, and our personalities mesh well together. I like to run scenes quickly, and move patients to the ambulance, so the fire crews can go back in service and get back to their games of checkers. Slimm just wants to take people to the hospital.
Slimm laughs at my jokes, too. Which helps.
Plus, he drives as smooth as butter. It will be a sad day when Slimm gets moved.
Sunday, August 21, 2011
Those pockets aren't for your hands...
So, Slimm and I had a student third rider the other day. I enjoy having students, I really do. They are, for the most part, sponges for knowledge, tend to ask good questions, and are generally helpful. This one was none of the above.
I'll call him Goofus.
My partner and I started this shift as usual, with a check-off sheet in our hands. Goofus had failed to introduce himself at this point, and stood about 20 feet to the side, with his hands in his pockets. We were prepared to leave him standing there in the parking lot, but he managed to sneak in the side before we could drive off. Then he took a nap.
Granted, this is an early-starting shift, but beginning the shift by napping in the back does not bode well for the rest of the day.
The day started off plainly enough, with a vent transfer from a long-term hospital to another hospital's ICU, then with some driving from post to post, then finally, a call. It turned out to be nothing, with no assistance from the fire department needed or wanted. What was of note, however, was that Goofus kept his hands in his pockets. The entire call.
The rest of the shift was utterly boring. Some schizophrenic man with diarrhea for a week, and no shoes, a known alcoholic drug-seeker with abdominal pain and an incredibly steep and long driveway, and some other calls that were bland to the point of not remembering. Goofus never took his hands out of his pockets, never spoke to the patients, never attempted an assessment, much less an intervention, didn't participate in the hand off of patients to nurses, and didn't help my partner or I put the truck back together in preparation for the next run.
As we were handing off the ambulance to the oncoming crew, Goofus had the nerve to ask me if I would go into the monitor archives and print vitals for all the patients we had transported.
I'm not sure if Goofus ever got his vitals, or if Goofus ever got anyone to sign his paperwork for school. I am pretty confident, however, that Goofus will have a very short, if any, career in EMS.
I'll call him Goofus.
My partner and I started this shift as usual, with a check-off sheet in our hands. Goofus had failed to introduce himself at this point, and stood about 20 feet to the side, with his hands in his pockets. We were prepared to leave him standing there in the parking lot, but he managed to sneak in the side before we could drive off. Then he took a nap.
Granted, this is an early-starting shift, but beginning the shift by napping in the back does not bode well for the rest of the day.
The day started off plainly enough, with a vent transfer from a long-term hospital to another hospital's ICU, then with some driving from post to post, then finally, a call. It turned out to be nothing, with no assistance from the fire department needed or wanted. What was of note, however, was that Goofus kept his hands in his pockets. The entire call.
The rest of the shift was utterly boring. Some schizophrenic man with diarrhea for a week, and no shoes, a known alcoholic drug-seeker with abdominal pain and an incredibly steep and long driveway, and some other calls that were bland to the point of not remembering. Goofus never took his hands out of his pockets, never spoke to the patients, never attempted an assessment, much less an intervention, didn't participate in the hand off of patients to nurses, and didn't help my partner or I put the truck back together in preparation for the next run.
As we were handing off the ambulance to the oncoming crew, Goofus had the nerve to ask me if I would go into the monitor archives and print vitals for all the patients we had transported.
I'm not sure if Goofus ever got his vitals, or if Goofus ever got anyone to sign his paperwork for school. I am pretty confident, however, that Goofus will have a very short, if any, career in EMS.
Saturday, August 20, 2011
We have to start somewhere
Admittedly, I am a blogging idiot. My expertise and experience centers on the reading of others' writings.
Those other blogs out there have served to provide me with some good inspiration, as do the seemingly endless number of dumbasses I encounter in life. I have often said that "I don't like people," which typically gets a humorous response. The fact is, I love people. From a distance. Like, through my television.
I am planning on writing on EMS as viewed from my ambulance, through my eyes. I will try to keep my comments and posts relevant to topics and trends in EMS, but occasionally, something awesome happens totally unrelated to EMS, such as Bubba Watson reaching a 667 yard par-5 in 2. That guy is a S-T-U-D.
They say any journey begins with the first step. This is mine.
Those other blogs out there have served to provide me with some good inspiration, as do the seemingly endless number of dumbasses I encounter in life. I have often said that "I don't like people," which typically gets a humorous response. The fact is, I love people. From a distance. Like, through my television.
I am planning on writing on EMS as viewed from my ambulance, through my eyes. I will try to keep my comments and posts relevant to topics and trends in EMS, but occasionally, something awesome happens totally unrelated to EMS, such as Bubba Watson reaching a 667 yard par-5 in 2. That guy is a S-T-U-D.
They say any journey begins with the first step. This is mine.
Subscribe to:
Posts (Atom)